Medications for Chronic Pain Treatment
Medications for Chronic Pain Treatment
Why I say there are no medications that cure chronic pain, how I prescribe them, and how to ask your doctor the right questions
01 Why I say there are no medications that cure chronic pain
Improper use of painkillers is my concern. I understand that people come to the doctor for a prescription not for pleasure. And doctors prescribe not for their own enjoyment.
To treat pain, it is important to understand the mechanism.
Acute pain is an alarm signal. Chronic pain is when the alarm signal is stuck in the “on” position, even though the fire has long been extinguished.
Chronic pain is a special state of the nervous system where pain pathways in the brain become overly sensitive, the pain threshold lowers, and the brain starts generating pain often without obvious physical damage. This is not “all in your head” in the usual sense. These are real neuronal changes visible on MRI.
A pill can mute the signal. But it cannot retrain the nervous system. So once the effect wears off, everything goes back to normal.
02 Five ways to retrain the nervous system
The real work with chronic pain is retraining the nervous system. And it must simultaneously target five mechanisms:
Psychology
CBT, hypnosis, working with catastrophizing, reinterpreting pain
Movement
Measured physical activity — the most powerful neuroplastic tool
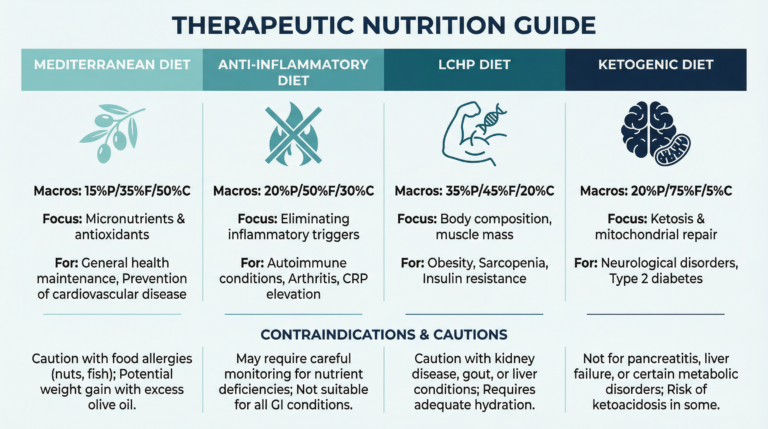
Nutrition and Biochemistry
Anti-inflammatory diet, correction of deficiencies that amplify pain
Lifestyle
Sleep, stress, daily rhythm — all directly affect pain threshold
Motivation
Without it, the other four don’t work. This is not a cliché, but neurobiology
Medications are intentionally absent from this list as they are only an auxiliary tool.
03 When medications make sense
Sometimes the pain is so severe that a person simply cannot start working, move, think, or sleep. In such cases, I sometimes prescribe medications. Not to cure the pain, but to create a window of opportunity for real work.
Sometimes chronic pain is closely intertwined with depression or sleep disorders. Sometimes psychotherapy and lifestyle adjustments help. Sometimes medication support is necessary. And this is always a very complex decision that must be made by the doctor together with the patient.
💡 Key idea: a pain medication is not a cure, it’s scaffolding. It’s needed while the building is being constructed. Then it’s removed.
04 “Here and now” vs “long and serious”: two types of drugs
Before we move on to specific names, it’s important to understand the logic. All pain medications can be roughly divided into two fundamentally different classes:
“Here and now” painkillers
Their goal is to relieve pain at a specific moment. Paracetamol, Analgin, Optalgin. NSAIDs: ibuprofen, diclofenac, brexin, etopan, arcoxie, etc. Opioids — natural (poppy alkaloids: morphine, codeine), semi-synthetic (morphine derivatives), and synthetic (methadone, fentanyl). They can help in an acute episode but do not change the system itself. With constant use, there is a high risk of dependence and so-called “abuse pain”: when the painkillers themselves provoke pain.
Medications for chronic pain treatment
Their goal is to change how the nervous system processes pain signals. They do not relieve pain instantly. They work cumulatively, over weeks. And their mechanism is completely different.
There is another type — local anesthetics, but we will discuss them in a separate post.
05 Medications used for chronic pain treatment
They are less known and raise many questions among patients. Let’s try to understand.
Pregabalin
Lyrica, Algerica, PregabinWhat it is: an antiepileptic drug that “calms” overexcited nerve cells. It reduces excessive activity of pain neurons, as if turning down the volume on an overloaded amplifier.
Relation to pain: in chronic pain, the nervous system “overheats,” neurons are easily excited. Pregabalin raises the pain sensitivity threshold. It may help with neuropathic pain, fibromyalgia, post-herpetic pain.
Is it a narcotic? No. But it is a prescription drug with several side effects: drowsiness, dizziness, sometimes swelling. It is discontinued gradually, not abruptly.
Gabapentin
Neurontin, GabagammaWhat it is: the “younger brother” of pregabalin. The same mechanism — calming overexcited nerve cells, but slightly less potent and with a different side effect profile.
Relation to pain: neuropathic pain, post-surgical pain, restless legs syndrome. Often prescribed when pregabalin is unsuitable or contraindicated due to chronic diseases.
Is it a narcotic? No. Prescription-only, requires dose adjustment.
Duloxetine
Cymbalta, Duloxin, IlatrolWhat it is: an antidepressant from the SNRI group.
Relation to pain: serotonin and norepinephrine are not only “mood hormones.” They participate in the descending pain control systems in the spinal cord. Duloxetine enhances these systems, and the brain better “inhibits” pain signals from below. This is a completely separate mechanism from its antidepressant effect.
If the doctor prescribed an antidepressant, does it mean you have depression? Not necessarily. Although chronic pain and depression often go hand in hand, and duloxetine works on both fronts simultaneously. But it is also used for pain without depression, specifically as an analgesic.
Amitriptyline
Elavil, ElatrolWhat it is: one of the oldest antidepressants — tricyclic. In psychiatry, it has been mostly replaced by more modern drugs. But in chronic pain treatment, it unexpectedly turned out very valuable, especially in small doses not used for depression treatment.
Relation to pain: blocks several pain pathways simultaneously, improves sleep (which itself reduces pain), works for neuropathy, migraine, fibromyalgia.
Is it a narcotic? No. Many side effects: dry mouth, drowsiness, constipation, effects on the heart. Therefore, it is selected carefully, especially in the elderly.
06 Table: prescription, OTC, dependence
| Medication | Pain type | Prescription | Dependence |
|---|---|---|---|
| Paracetamol (Akamol, Panadol), Optalgin, Analgin | Acute, mild | OTC | No. Up to 3 weeks |
| Ibuprofen, diclofenac, etopan, arcoxie, brexin (NSAIDs) | Acute, inflammatory | OTC* | No. Up to 2-3 weeks |
| Pregabalin (Lyrica) | Neuropathic, chronic | Prescription | Rare. Long-term use |
| Gabapentin (Neurontin) | Neuropathic, chronic | Prescription | Rare. Long-term use |
| Duloxetine (Cymbalta) | Chronic, neuropathic | Prescription | No. Long-term use |
| Amitriptyline | Neuropathic, migraine | Prescription | No. Long-term use |
| Opioids (tramadol etc.) | Severe acute / oncologic | Strict prescription | High risk. Only a few days for acute pain (exception — palliative care) |
* Some NSAID dosages require a prescription. Check with your pharmacist.
07 Over-the-counter does not mean safe as candy
⚠️ This is important
Just because a medication is sold over the counter does not mean you can take it by the handful indiscriminately. Paracetamol in large doses is toxic to the liver. NSAIDs with long-term use pose risks to the stomach, kidneys, and heart.
Over-the-counter means only one thing: the government considers that with proper use this medication is safe enough for self-administration. The key words are “with proper use.”
That’s why even for OTC medications it’s worth talking to your doctor. Not to ask permission, but to ask the right questions.
08 The right questions to ask your doctor. Checklist
These questions will help you avoid mistakes when using medications.
Ask your doctor
Save or print and bring to your appointment